Stapedectomy
Description
Stapedectomy is the removal of a fixed stapes bone with the formation of a hole (stapedotomy) in the stapes footplate (oval window) in order to insert a piston-shaped prosthesis to reestablish adequate conduction of sound from the incus to the inner ear.
Indications for Surgery
Unilateral or bilateral otosclerosis causing progressive conductive hearing loss with minimal benefit from amplification.
Contraindications to Surgery
- Medical comorbidities that would preclude surgical or anesthesia risk
- Ongoing infection (otitis media or otitis externa)
- Active Ménière's disease
- Surgery is not recommended if the ear to be operated on is the better-hearing or only hearing ear
- Caution is advised when considering surgery in patients with other coexisting or precedent otologic conditions, including tympanic membrane perforation, cholesteatoma, or severe Eustachian tube dysfunction
Pre-Operative Evaluation
- Audiometric evaluation, including pure tone audiogram and acoustic reflex testing
- A computed tomography (CT) scan may be useful in identifying otosclerosis (thickening of the stapes
footplate may be seen), as well as anatomic anomalies that may affect surgical planning, such as an
abnormal course of the facial nerve. However, a negative CT scan does not exclude otosclerosis.
Anesthesia
General, although local anesthesia is also common.
Surgical Technique
- The patient is placed supine on the operating table and general anesthesia is induced via laryngeal mask airway.
- The table is rotated 180 degrees and the ear is prepped and draped.
- The external auditory canal is injected with 1% lidocaine with 1:100,000 epinephrine.
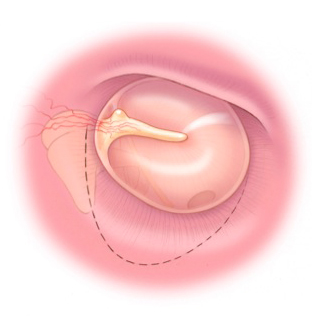
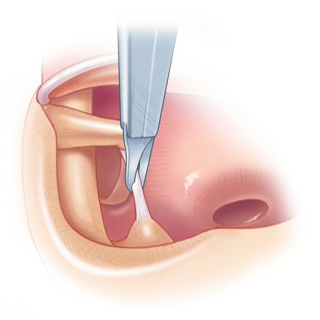
- A lateral incision is made in the canal approximately 4-8 mm away from the annulus. The incision is extended in the 12 o'clock direction to the malleus, and inferiorly to the 6 o'clock position.
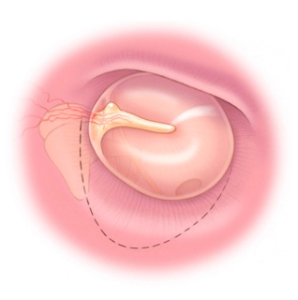
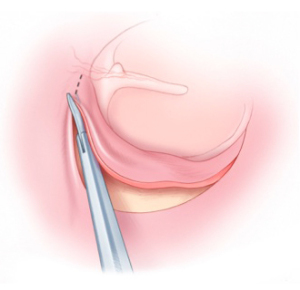
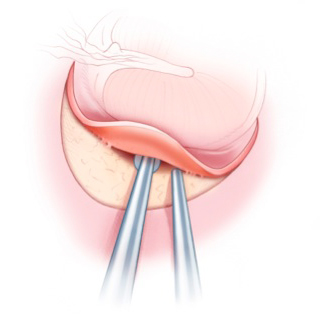
The tympanomeatal flap is then elevated.
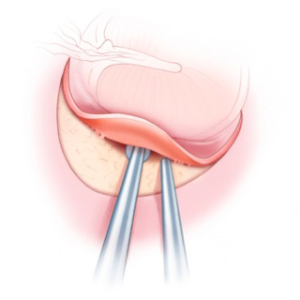
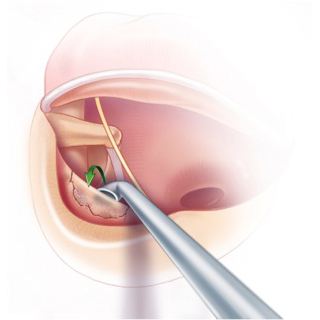
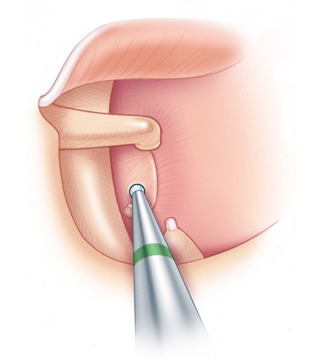
- The scutum is taken down using a diamond bur or a stapes curette until the pyramidal eminence, from which the stapedius tendon arises, is visualized posteriorly and the facial nerve is seen superiorly.
The chorda tympani is identified and preserved.
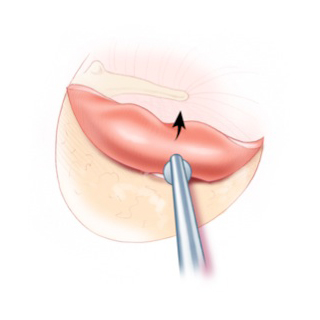
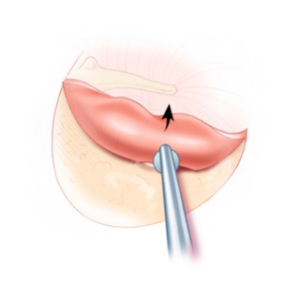
- The ossicular chain is palpated and fixation of the stapes confirmed.
- The distance between the oval window and the incus is measured and the appropriately sized prosthesis is selected.
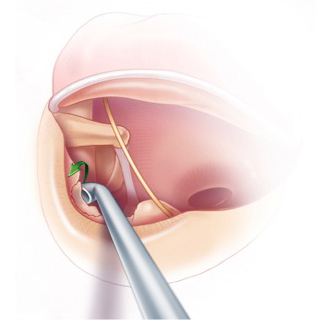
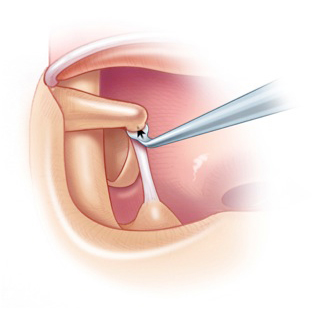
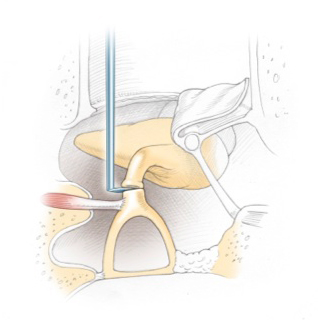
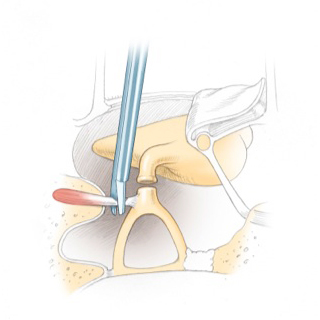
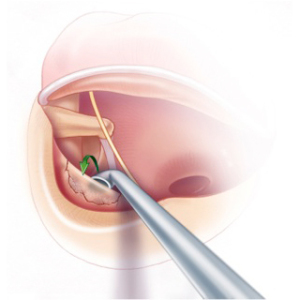
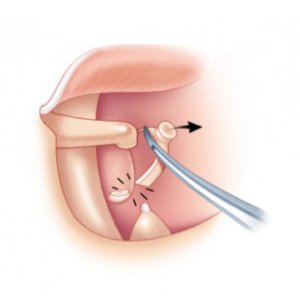
- The incudostapedial joint is severed using a knife,
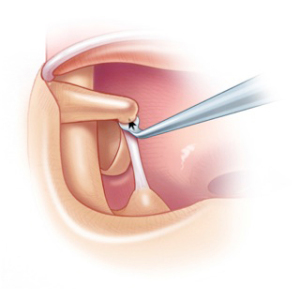
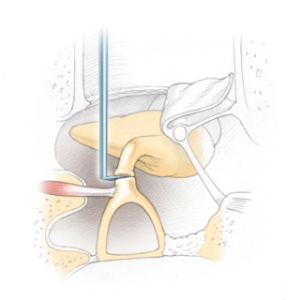
and scissors are used to sever the stapedius tendon.
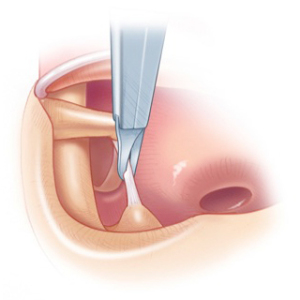
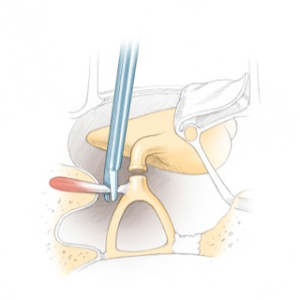
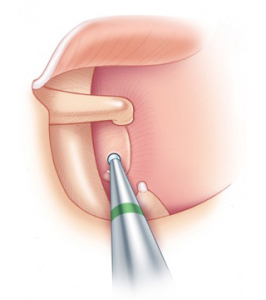
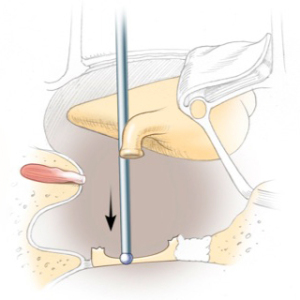
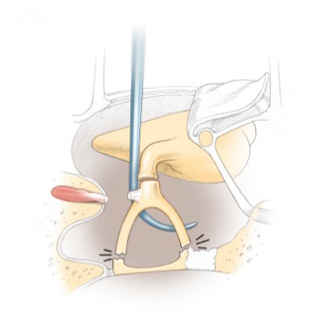
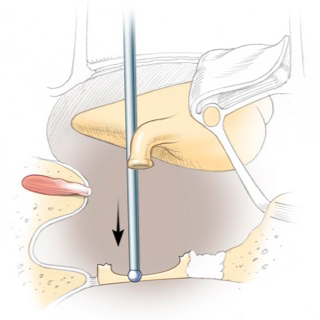
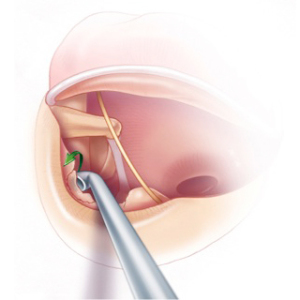
- The stapes superstructure is fractured towards the promontory.
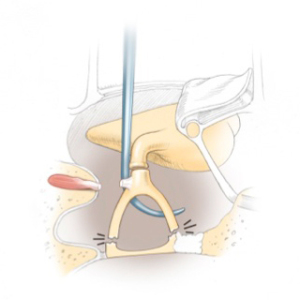
- A stapedotomy fenestra is made using a 0.7mm diamond bur or using a KTP laser.